
Gastrointestinal Bleeding
Gastrointestinal (GI) bleeding refers to any form of bleeding that occurs in the digestive tract, from the esophagus to the rectum. It is not a disease itself but a symptom of an underlying condition in the gastrointestinal system. GI bleeding can range from mild and chronic to severe and life-threatening, requiring prompt medical attention. It is broadly classified into upper GI bleeding (originating from the esophagus, stomach, or duodenum) and lower GI bleeding (from the small intestine, colon, or rectum).
Causes of Gastrointestinal Bleeding
Cholecystectomy is typically recommended when gallstones cause symptoms or complications. Common reasons include:
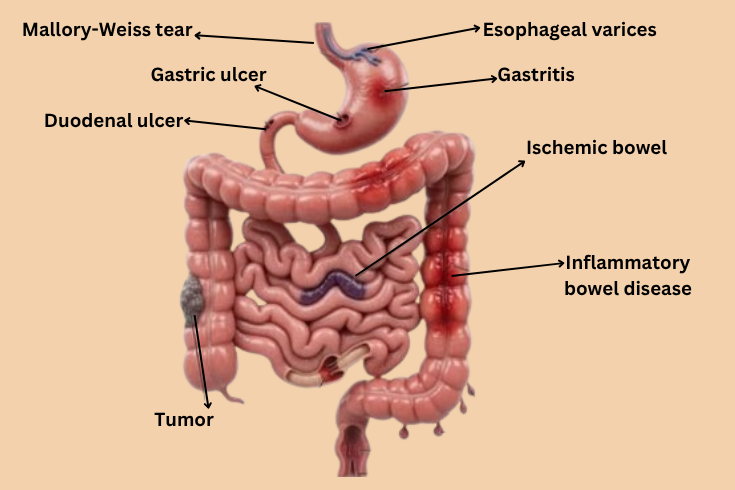
The causes differ based on the location of the bleed. Common causes of upper GI bleeding include peptic ulcers (often due to H. pylori infection or long-term use of NSAIDs like aspirin or ibuprofen), esophageal varices (enlarged veins in the esophagus, frequently linked to liver cirrhosis), gastritis, and Mallory-Weiss tears from severe vomiting.
Lower GI bleeding is commonly caused by diverticular disease, where small pouches in the colon wall bleed when inflamed or eroded. Other frequent causes include hemorrhoids, colorectal polyps or cancer, inflammatory bowel disease (such as Crohn’s disease or ulcerative colitis), and angiodysplasia (abnormal blood vessels in the intestinal lining).
Risk factors that increase the likelihood of GI bleeding include advanced age, use of blood-thinning medications, chronic liver disease, alcohol consumption, and a history of gastrointestinal disorders.
Symptoms of Gastrointestinal Bleeding
1
Symptoms vary depending on the site and severity of the bleeding. In upper GI bleeds, patients may experience vomiting blood (hematemesis), which can appear bright red or like coffee grounds, along with black, tarry stools (melena) due to digested blood. Lower GI bleeds often present with bright red blood in the stool (hematochezia) or maroon-colored stools.
2
Chronic or occult (hidden) bleeding may not show visible blood but can lead to symptoms of anemia, such as fatigue, weakness, shortness of breath, dizziness, pale skin, and rapid heartbeat. Severe bleeding can cause abdominal pain, fainting, confusion, or shock if significant blood loss occurs. Early recognition of these signs is crucial for timely intervention.
Diagnosis and Management
Diagnosis begins with a thorough medical history and physical examination. Doctors may order blood tests to check for anemia, clotting issues, or liver function. Stool tests can detect hidden blood. The primary diagnostic tools are upper endoscopy (EGD) for upper GI issues and colonoscopy for lower GI bleeding. These procedures allow direct visualization of the bleeding site and often enable immediate treatment, such as clipping, cauterizing, or injecting medications to stop the bleed.
In some cases, imaging like CT angiography or capsule endoscopy may be used for obscure bleeding sources. Initial management focuses on stabilizing the patient with intravenous fluids, blood transfusions if needed, and medications like proton pump inhibitors (PPIs) to reduce stomach acid in upper GI cases.
Advanced surgical gastroenterology plays a key role in managing complex or recurrent GI bleeding, especially when linked to tumors, severe ulcers, or structural issues. Minimally invasive laparoscopic techniques and endoscopic interventions provide effective control with faster recovery and reduced complications.
Conclusion
Gastrointestinal bleeding is a serious condition that demands immediate evaluation to identify and treat the underlying cause. While many cases resolve with conservative or endoscopic management, persistent or heavy bleeding requires expert intervention to prevent complications like severe anemia or hemodynamic instability. Adopting a healthy lifestyle, avoiding excessive NSAIDs and alcohol, and seeking prompt care for persistent digestive symptoms can help reduce risks. Early diagnosis and appropriate management significantly improve outcomes and quality of life for patients experiencing GI bleeding